



Mini Review
Moudni S*, Moussaoui H., Mouhibi A., Andoh A
Correspondence Address :
Moudni S (2022)
Fixed Prosthesis Department,
Faculty of Dentistry of Casablanca,
Hassan II University of Casablanca,
Morocco
Received on: October 20, 2022, Accepted on: November 28, 2022, Published on: December 02, 2022
Citation: Moudni S, Mouhibi A., Moussaoui H., Andoh A (2022). WAX-UP: Interests and Techniques
Copyright: © 2022, Moudni S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Diagnostic wax-ups are not routine procedures because they are time-consuming and do not result in immediate tangible benefits. Nonetheless, a diagnostic wax-up is one of the most useful diagnostic techniques for patients seeking fixed prosthodontics. Awkward edentulous spaces, reverse articulation, difficult tooth- ridge relationships, and the need for atypical contours often are first discovered during this waxing procedure [1].
Wax-up or diagnostic wax-up is the dental diagnostic procedure that allows the planning of restorations using wax and the prefiguration of the desired contours of the teeth on plaster models before preparation [2].
In the laboratory, the production of diagnostic waxes can be done either by traditional, subtractive or additive techniques or by new virtual techniques [3].
The objective of this work is to define the interests of diagnostic waxes as well as to describe the different methods of their manufacture.
Wax-up interests
In the diagnosis:
- Provide information on the need for coronoplasty, depulpation or coronaryelongation.
- Guide the choice of the type of surgical intervention to be performed [4].
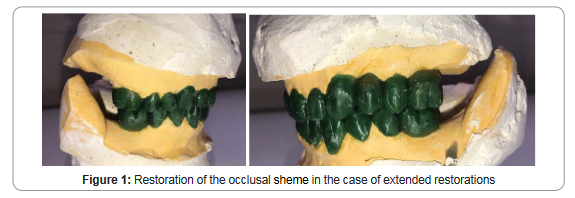
- Specify the occlusal sheme by redrawing the occlusal curves, redefining the DVO as well as the meshing, in the case of extended restorations (figure 1).
In pre-prosthetic therapy:
• Pre-prosthetic occlusal arrangements:
The realization of the diagnostic wax after the mounting of casts on articulator, allows a better evaluation of the occlusion and avoid any interference during the mandibular movements, creates an anterior guide and allows the modification of an altered curve of Spee [5].
• Realization of the provisional prosthesis: The provisional restoration reproduces the contours of the diagnostic wax-up.
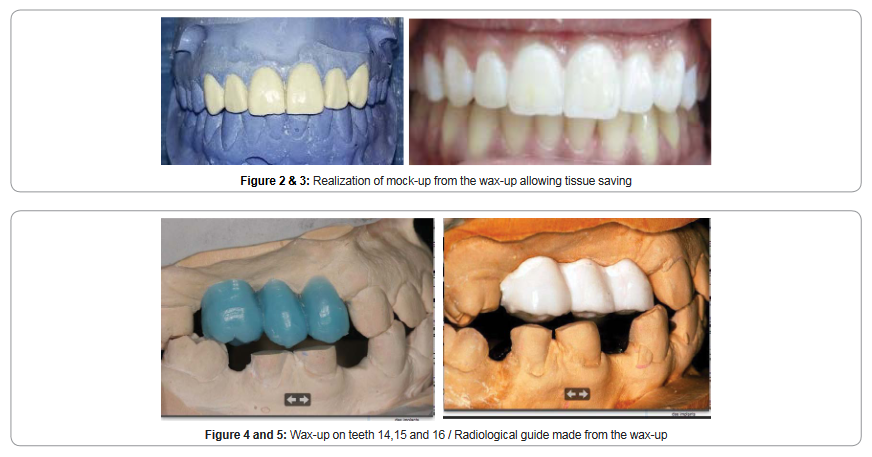
• In the case of aesthetic veneer restorations:
The wax-up allows to preview the final result by making aesthetic models (mock- up) (figure 2 and 3). It also allows the creation of a preparation guide which allows the practitioner to make preparations from the final volume of the restoration, preserving the enamel and not preparations from the existing surface of the tooth [5].
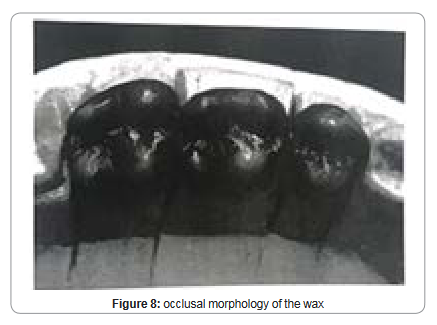
In the pre-implant study:
The wax-up makes it possible to produce the radiological and surgical guides in order to assess the available bone volume and the feasibility of the implant treatment (figure 4 and 5) [6].
Wax-up techniques
Conventional techniques:
The wax model must represent the desired shape of the final prostheses. It can be made in wax or resin on the study model [7]. The necessary material for its realization can be summarized in: a plaster working model, a bristle brush N 10, zinc stearate, pencils of various colors, a heat source, inlay wax sticks, a ceramic slotted paddle, a PK Thomas instrument kit and addition instruments [8]. There are two techniques described for making wax-ups;.
H.C.LUNDEEN’s method: first diagnostic wax technique developed with the aim of restoring occlusal contacts. It goes through several stages:
1- Functional and non-functional cuspids are located. The wax cones for each cuspid are placed by the PKT n1 (figure 6) [9]
2- The marginal and axial ridges are added with the same instrument (figure 6) [9]
3- Adding the triangular ridges, then developing the axial contours with the PKT n 4 (figure 7) [9]
4- Finally, the grooves are smoothed with PKT n3 and the marginal ridges with PKT n5 (figure 8) [9]
5- Softening of occlusal surfaces with zinc stearate [9]
6- the contacts formed by each opposing cuspid must form a tripodic configuration [9]
7- Finishing touches [9]
PK.THOMAS’s method: aiming for the development of a cuspid-to-fossa occlusion that allows a balanced occlusion. It is performed in several steps:
1- The location of the cuspids and the contacts made by them are identified and marked on the casts.
2- The cones are first placed for the mandibular functional cuspids.
3- Then the cones are placed for the maxillary palatal cuspids.
4- Non-functional cuspids are placed.
5- Marginal ridges and cuspid ridges are developed for opposing teeth.
6- Softening of occlusal surfaces with zinc stearate.
7- Finishing touches (9)
Virtual wax-up:
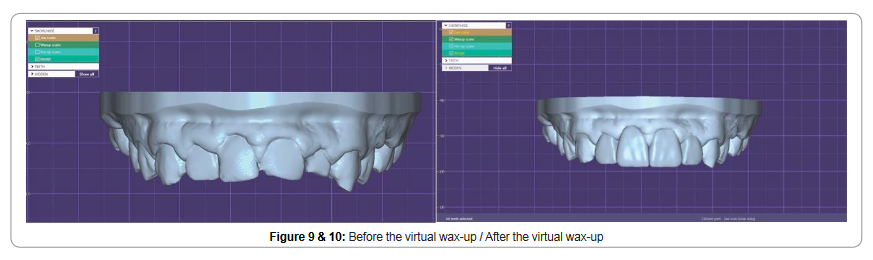
Before preparation:
The virtual wax-up is similar to the conventional wax-up. Its realization is done during the preoperative phase by some systems (ex: 3shape). It is a question of first carrying out the facial and intra-oral digitization of the patient using the optical impression, then thanks to the design tools, the visualization of the project on the virtual model is obtained by respecting the morphology of the teeth, the occlusal context and the aesthetic references of the face (figure 9 and 10). Once made, this virtual wax-up is made concrete using the 3D printer (stereolithography) generally in calcinable resin. At this stage, the wax-up can therefore be tried and validated in the mouth even before preparation [10].
After preparation:
After scanning the model (or impression), the margin line of the preparation(s) is determined either automatically or manually. A manual correction of the limit makes it possible to adjust the automated determination of this one, using the mouse of the computer, each point of the limit can then be modified by computer. A diagnostic wax (wax up) is offered by the software thanks to a database of dental morphologies which can be modified, allowing the prosthetic project to be visualized [10]. It is often recommended to carry out an aesthetic study beforehand and then to scan the clinically validated diagnostic waxes before modeling. This stage of adjustment of the diagnostic waxes will allow the homothetic reduction of these waxes. The cuffs for adjustment and modification of the shape (or morphing) allow certain anatomical corrections of the future prosthetic part [5].
Conclusion
The realization of a prosthetic restoration adapted to the occlusion, the function, the aesthetics and the periodontal requirements passes necessarily by a fundamental stage of laboratory which is the modification of initial casts by a wax construction aiming at representing the final state of the therapy.Today, digitalization is omnipresent in dentistry. Thanks to these new tools, a field of new possibilities has opened up. To produce a provisional prosthesis, modeling, which is the fourth step of indirect CAD/CAM, uses a diagnostic wax proposed by a software that allows the visualization of the prosthetic project. This method of realization of aesthetic projects has several advantages compared to traditional techniques especially in the notion of saving time and precision.
1. Deborah L., M. Harry Parker, S. Cameron. Quick chairside diagnostic wax- up. J Prosthet Dent. 2022;87(5):581-2.
2. Clément M, Noharet R, Vionnet S. Réalisation clinique d’une prothèse fixée unitaire Encyc. Med. Chig. Odonto 2015;
3. Ara Na. Enhancing a Smile with Cosmetic Dentistry in the New Economy Dent. Econom. Sep 2013.
4. Laura K, Juan O. An Advanced Diagnostic wax-up. J. of Cosmetic. Dent. 2010. Summer 2010.
5. Cyril GAILLARD. Technique de prévisualisation : projet esthétique et guidede préparation dentaire. Le Fil Dentaire N° 93 • mai 2014.
6. J-P. Lacoste. Guide radiologique, guide chirurgical Guide pratique d’implantologie 2013.
7. Harel S, Pascal M. Clinically Based Diagnostic wax-up for optimal Esthetics. J Calif. Dent. Assoc. 2008;36(5):355-362.
8. Romerowski J, G. BRESSEN. Utilité de la technique de la cire par addition en anatomie dentaire. Encyc. Med. Chig. Stomato. 22-003-P-30-2008.
9. Mulay G, Dugal R. Waxing technique to develop proper occlusal morphology in different occlusal shemes. J. Indian. Prosthod. Soc. 2011;11(4):205-209.
10. Hollender M, Allard Y, Richelme J, Casu J P la CFAO indirecte. L’INFORMATION DENTAIRE n° 20 - 21 mai 2014.



Clinical Microbiology & Case Reports

Women's Health & Gynecology

Journal of Global Diabetes & Clinical Metabolism

Journal of Alzheimers Parkinsonism and Dementia
Journal of Dental and Oral Health

Journal of Ophthalmology & Visual Neuroscience

Cancer Science: Open Access

Journal of Immunology, Infection & Inflammatory Diseases

Journal of Prevention & Treatment of HIV/AIDS

Journal of Primary Health Care & General Practice

Journal of Blood Disorders Symptoms and Treatments

Journal of General and Emergency Medicine

Journal of Clinical Anesthesia and Pain Medicine

Journal of Applied Physics & Nanotechnology

Journal of Advances in Breast Cancer Research and Development

Interdisciplinary Journal of Gastroenterology, Hepatology and Endoscopy

Journal of General Surgery

Journal of Global Vaccines R&D

Journal of Integrative Pediatric Healthcare: Open Access

SOA-Clinical & Medical Case Reports, Reviews

Interdisciplinary Journal of Bone Marrow & Stemcell

Interdisciplinary Journal of Nursing and Critical Care

Global Journal of Internal Medicine

Journal of Integrative Food Sciences & Nutrition

Integrative Clinical Cardiology

Clinical Dermatology and Investigations

Molecular Medicine: Current Aspects

Open Access Journal of Public Health (ISI Indexed)

Annals of Clinical Research and Trials

Global Chemical Engineering & Process Technology

Integrative Plant Science & Molecular Biology

Interdisciplinary Journal of Translational Science

Integrative Neurology and Stroke

Journal of Vascular Diseases and Therapy

Integrative Trauma and Emergency Medicine

SOA-Otolaryngology-ENT Research

Global Urology and Nephrology

Journal of Pregnancy and Newborncare

SOA-Applied Biotechnology & Bioengineering

Journal of Obesity Treatment and Weight Management

SOA Medical Research & Clinical Practice

Integrative Clinical Pathology

Global Toxicology

Dairy Science, Veterinary and Animal Husbandry

SOA Radiology & Radiation Therapy

Global Analytical Techniques & Pharmaceutical Research

Abnormal Psychology and Clinical Psychiatry

SOA Archives of Pharmacy & Pharmacology

Global Nutrition and Dietetics

Global Hydrologic Engineering Research

Global Physical Medicine & Rehabilitation Practices

Integrative Oral care and Craniofacial Research
Integrative Ecology and Environmental Sciences

Open Access Journal of Sociology
Interdisciplinary Journal of Fisheries and Aquaculture research
Biomedical Research and Clinical Studies

Clinical Epidemiology and Healthcare

Molecules Research & Analysis
Journal of Polymers Research










 Open Access
by Scient Online is licensed.
Open Access
by Scient Online is licensed.

